Weight Loss and Sleep Apnea: How BMI Directly Impacts CPAP Pressure Needs

Feb, 3 2026
Why Your Weight Matters More Than You Think for Sleep Apnea
If you’re using a CPAP machine and still feel tired in the morning, the issue might not be the machine-it could be your weight. Obstructive sleep apnea (OSA) isn’t just a breathing problem. It’s deeply tied to how much fat your body carries, especially around your neck, chest, and belly. For every 1-point drop in your BMI, your breathing interruptions during sleep go down by about 6.2%. That means if you lose 7 pounds, you’re likely to see a 7% reduction in apneas. Sounds simple? It is. But most people don’t realize how powerful that number is.
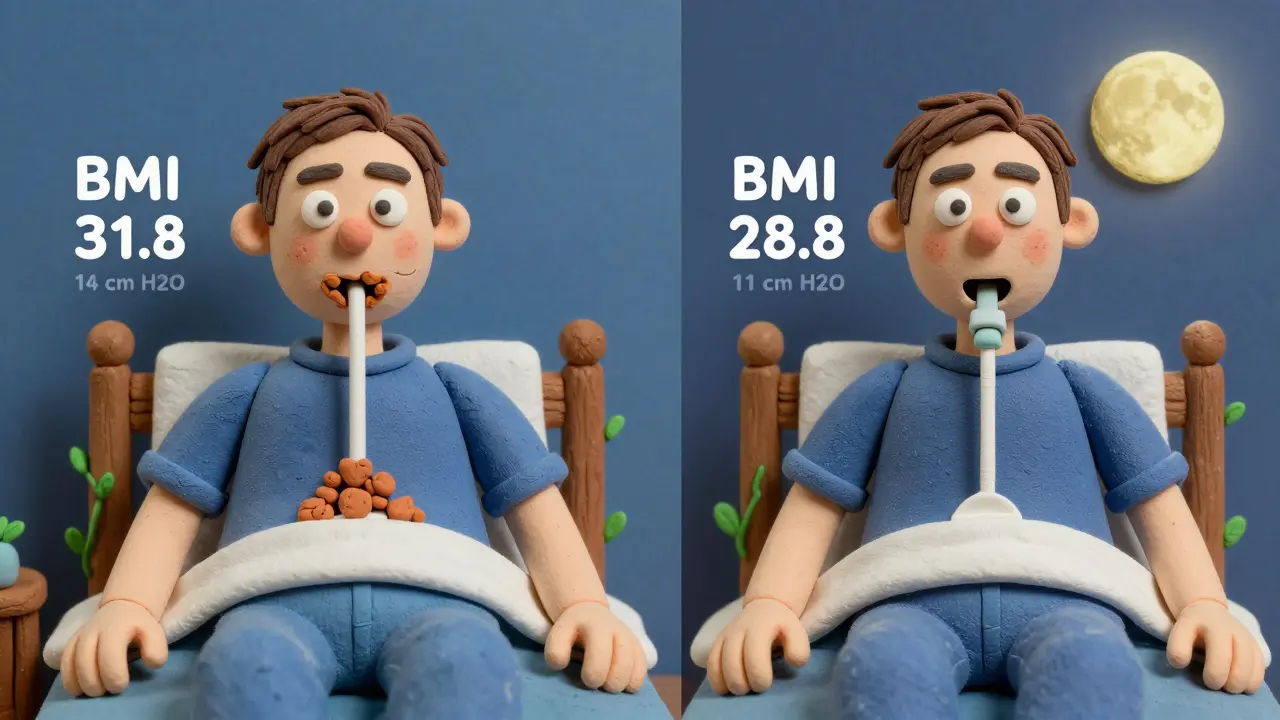
Take a man who’s 5’10" and weighs 220 pounds. His BMI is 31.8. His CPAP is set at 14 cm H2O because his airway collapses too easily. If he loses 20 pounds, his BMI drops to 28.8. That’s a 3-point change. Based on research from Fattal et al. (2022), his apnea-hypopnea index (AHI) could drop by nearly 20%. For some, that’s enough to switch from moderate to mild OSA. For others, it means they can lower their CPAP pressure-or even stop using it altogether.
How Extra Weight Squeezes Your Airway
It’s not just about being “heavy.” Fat doesn’t just sit on your skin-it settles where it matters most for breathing: around your neck, inside your chest, and on your abdomen. That extra tissue pushes down on your windpipe, making it harder to keep open while you sleep. A neck circumference over 17 inches in men (or 16 inches in women) is a red flag, even if your BMI is only in the overweight range.
Here’s the scary part: the more fat you carry, the higher the CPAP pressure your machine needs to force air through. Most devices work between 4 and 20 cm H2O. Normal-weight patients often need just 8-10 cm H2O. But someone with a BMI over 35? They’re often set at 14-20 cm H2O. That’s like trying to blow air through a straw packed with cotton. The machine has to work harder-and so does your body.
The CPAP Weight Gain Paradox
Here’s where it gets confusing. CPAP therapy fixes your breathing. You sleep better. You wake up less tired. So you think, “Great, now I can eat more.” And many people do. Studies show that after starting CPAP, people report eating 287 more calories a day on average. Your body also starts burning fewer calories-basal metabolic rate drops by 5.3% in some cases.
This is the paradox: CPAP helps you breathe, but it can make you gain weight. Why? Because untreated OSA raises ghrelin (the hunger hormone) and lowers leptin (the fullness signal). When CPAP fixes your sleep, those hormones reset. But if you don’t change your eating habits, you gain weight. One study found that patients using CPAP less than 5 hours a night gained an average of 1.8 kg in six months. Those who used it consistently? Only 0.3 kg.
It’s not the machine’s fault. It’s the behavior around it. If you’re sleeping better but still eating fast food and sitting on the couch, you’re setting yourself up for weight gain. That’s why CPAP alone isn’t a cure-it’s a tool. And tools need direction.
How Much Weight Do You Actually Need to Lose?
You don’t need to lose 50 pounds to see results. Losing just 5-10% of your body weight can cut your apnea events in half. For someone who weighs 200 pounds, that’s 10-20 pounds. That’s not a miracle. That’s a realistic goal.
Research from the Obesity Medicine Association shows that 37% of patients with OSA see their apnea resolve completely after intensive lifestyle changes. But 78% of those who had bariatric surgery saw their OSA vanish. That’s not a coincidence. It’s biology. Fat around the airway melts faster than fat elsewhere. Even if you don’t see your scale drop dramatically, your neck circumference might shrink. And that’s what matters most.
One patient from Sydney, a 42-year-old woman with a BMI of 38, lost 18 pounds over 8 months. She didn’t change her diet drastically-just cut out sugary drinks and started walking 30 minutes after dinner. Her CPAP pressure dropped from 16 cm H2O to 11. Her AHI went from 28 to 8. She no longer needed to sleep on her side. She stopped snoring. Her husband noticed.
CPAP Pressure and BMI: The Math Behind the Machine
There’s a direct formula doctors now use: for every 1-point increase in BMI, CPAP pressure needs to rise by about 0.5 cm H2O to keep the airway open. So if your BMI goes from 30 to 35, your pressure might need to jump from 10 to 12.5 cm H2O. That’s not guesswork-it’s based on data from over 400 patients in polysomnography studies.
That’s why newer CPAP machines, like ResMed’s AirSense 11 AutoSet for Her and Philips’ DreamStation 3, now have built-in BMI-calibrated algorithms. They don’t just deliver pressure-they adjust based on your weight trends. If you lose weight, the machine can sense it (if you log your weight) and lower pressure automatically. That’s huge. It means your treatment can evolve with you.
What Works Better Than Just CPAP?
CPAP is the gold standard-but it’s not enough by itself. The most successful patients don’t just use their machine. They combine it with:
- Weight loss goals: Aim for 5-10% of body weight. That’s your first target.
- Structured sleep: Go to bed and wake up at the same time every day. Consistency improves metabolic health.
- Protein-rich meals: Protein keeps you full longer and helps preserve muscle while losing fat.
- Walking after dinner: Just 20-30 minutes cuts nighttime apnea events by 15-20% in studies.
- Regular check-ins: See a sleep specialist and a dietitian together. One 2021 trial showed patients with coordinated care lost 42% more weight than those who got standard advice.
And don’t ignore the emotional side. Many people feel shame around their weight. But OSA isn’t a failure of willpower. It’s a medical condition worsened by biology. You’re not lazy. You’re stuck in a cycle. Breaking it takes support-not judgment.
When CPAP Isn’t Enough
If your BMI is over 40 and you’re still struggling with high pressure, poor mask fit, or constant leaks, CPAP alone might not be the answer. That’s when other options come in:
- Mandibular advancement devices: These mouthpieces reposition your jaw to open your airway. They’re less effective than CPAP for severe cases, but work well for mild to moderate OSA with weight loss.
- Hypoglossal nerve stimulation: A small implant that stimulates the tongue muscle to keep the airway open. It’s FDA-approved for patients with BMI 35-40 who can’t tolerate CPAP. Success rates? 71%.
- Bariatric surgery: For those with severe obesity, this is the most effective long-term solution. After gastric bypass, 78% of patients no longer have OSA after one year.
None of these are quick fixes. But they’re options. And they’re better than giving up.
Real People, Real Results
Reddit user u/SleepWarrior42 posted: “After losing 45 pounds from BMI 38 to 31, my AHI dropped from 32 to 9. My pressure went from 14 to 9 cm H2O. I only use CPAP now when I sleep on my back.”
Another patient, a 56-year-old teacher from Brisbane, lost 22 pounds over a year. Her CPAP pressure dropped from 18 to 12. She stopped taking blood pressure meds. Her doctor said her insulin sensitivity improved by 17%. She didn’t do keto. She didn’t join a gym. She just started eating dinner earlier and walking after.
These aren’t outliers. They’re proof that the numbers work. Lose weight. Lower pressure. Improve sleep. Break the cycle.
What to Do Next
Here’s your simple plan:
- Check your current BMI. Use a reliable calculator (height and weight only).
- Log your CPAP pressure setting. It’s on your machine’s report.
- Set a 5% weight loss goal. For a 200-pound person, that’s 10 pounds.
- Track your neck circumference monthly. Measure just below the Adam’s apple.
- Ask your sleep doctor for a follow-up sleep study after 6 months. If your AHI dropped by 50%, pressure reduction or discontinuation might be possible.
You don’t need to be perfect. You just need to move. Every pound lost is a step toward breathing easier. And that’s worth it.
Can losing weight cure sleep apnea?
Yes, for many people. Losing 5-10% of body weight can reduce apnea events by 50% or more. In some cases, especially with mild to moderate OSA, weight loss can eliminate the need for CPAP entirely. Studies show 37% of patients who lose weight through lifestyle changes no longer meet the diagnostic criteria for OSA. For those with severe obesity, bariatric surgery resolves OSA in 78% of cases after one year.
Does CPAP help you lose weight?
Not directly-but it creates the conditions for it. CPAP improves sleep, which lowers stress hormones like cortisol and restores balance to appetite-regulating hormones (leptin and ghrelin). This can reduce cravings and increase energy for activity. However, if you don’t change your diet, CPAP can lead to weight gain due to increased appetite and lower metabolism. The key is pairing CPAP with intentional lifestyle changes.
Why does my CPAP pressure keep going up?
If your BMI has increased since you started CPAP, your pressure likely needs to rise to keep your airway open. Each 1-point increase in BMI typically requires about 0.5 cm H2O more pressure. Weight gain from poor sleep, medication, or lifestyle changes can also raise pressure needs. Talk to your sleep specialist-your machine may need recalibration, or you may need to address underlying weight gain.
Can I lower my CPAP pressure if I lose weight?
Absolutely. Most patients who lose 10% of their body weight can reduce their CPAP pressure by 1-3 cm H2O. Some even eliminate the need for CPAP. But don’t adjust it yourself. Always get a follow-up sleep study to confirm your AHI is low enough before making changes. Pressure too low can cause apneas to return.
What’s the best way to lose weight if I have sleep apnea?
Start with small, sustainable changes: cut sugary drinks, eat dinner earlier, walk after meals, and get 7+ hours of sleep. Combine CPAP use with structured support-a sleep specialist and dietitian working together. Research shows this approach leads to 42% more weight loss than doing either alone. Avoid extreme diets. Focus on consistency, not speed.







